
This is the second in a series of six articles that will describe the foundation of evidence and thinking that served as a catalyst for the development and evolution of the Applied Learning and Evidence Translation (ALET™) Blueprint , first described in the 2025 White Paper titled “The Education We Deliver Isn't Built for the Change We Expect,”1 developed by the ALET ™ Collaboratory. Please check out the first article Bridging the Knowing-Doing Gap: The Applied Learning and Evidence Translation (ALET™) Blueprint for Clinical Behavior Change.
The continuing education for the health professions (CEHP) field has reached an inflection point. While we've become increasingly proficient at measuring satisfaction, awareness, knowledge and competence, these traditional metrics have not demonstrated value in capturing the full range of forces that actually move clinicians from learning to action.1 As clinical decisions grow more complex and context-dependent, the gap between what we measure and what matters has become impossible to ignore.
This was the central premise of a recent ALET™ (Applied Learning & Evidence Translation) Collaboratory webinar.2 This article presents an overview of the roadmap for CEHP professionals ready to evolve their measurement paradigm in step with their design intent, as described in the ALET™ Blueprint.1
The Fundamental Shift: From Education to Enablement
Clinicians today face decisions that are more complex, more contextual and more dependent on factors beyond knowledge: confidence, intent, commitment and real-world constraints all play critical roles in whether learning translates to practice change.
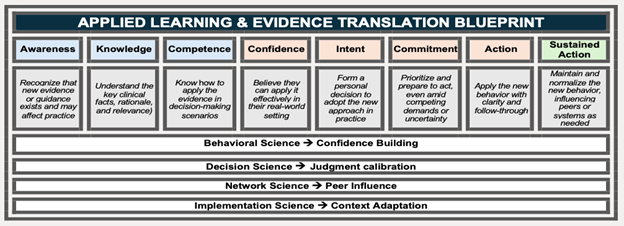
The ALET™ Blueprint, introduced in 2025, is an 8-stage framework that provides a cohesive model and shared language for the full clinician journey from awareness of new evidence to consistent application in real-world clinical practice.1 Grounded in behavioral science, decision science, network science and implementation science, the Blueprint acknowledges what frontline educators have long understood: The middle of the pathway (where clinicians move from knowing to believing to intending to actually taking first steps) has been woefully underdesigned and undermeasured in continuing education/continuing professional development (CE/CPD).
This gap leaves the community dependent on commonly used measures, including participation metrics, pre- and post-activity knowledge checks, and an assortment of quasi-validated subjective measures. However, in the evermore complex landscape of therapeutic options, CE/CPD must equip healthcare professionals with the performance-ready skills, confidence and clinical reasoning to enact care decision-making that is aligned with best evidence, in the service of high-quality and effective patient care. As noted in the recent webinar, when our design intent expands, our measurement also must expand.2 This effort isn't about discarding the foundation we've built through approaches such as the outcomes framework by Moore et al.3 This effort is focused on building on to this foundation and rising to the moment CE/CPD needs to meet for effective clinical care today.
The Four Critical Signals That Predict Real-World Change
Rather than proposing more metrics, the ALET™ framework introduces a different framework to offer visibility of enablement signals that more reliably predict whether a clinician will try something new, continue trying and successfully navigate application of learning into their specific clinical context. We believe four signals stand out as particularly relevant:
- Readiness
Readiness signals identify whether a clinician possesses not just knowledge, but the confidence and contextual capability required for early action. This signal captures perceived competence, emotional readiness and situational fit, which are the psychological and practical foundations that determine whether learning will translate to a first attempt. Readiness often breaks down not because clinicians lack knowledge, but because they lack confidence in their ability to navigate their specific environment. Traditional measures of knowledge and competence miss this entirely.
- Progression
Progression signals detect whether clinicians are actually moving from belief to preparation or transforming abstract agreement into concrete intent. The distinction here is crucial: Superficial expressions of interest ("that sounds like a good idea") differ fundamentally from genuine momentum toward action ("I can see exactly where this fits in my workflow next week"). Progression indicators help identify when momentum stalls, often revealing barriers invisible to traditional measurement approaches. A clinician might score perfectly on knowledge assessments while simultaneously recognizing their environment won't support the change, which is a critical insight that post-tests cannot capture.
- Commitment
Commitment signals capture the preparation phase, where clinicians begin aligning their environment for change. This stage is particularly vulnerable to breakdown, as it requires not just individual readiness but environmental and contextual readiness, which includes the support of colleagues, access to resources, alignment with workflows and/or institutional backing. Measuring commitment means detecting whether clinicians are taking concrete preparatory steps: Identifying specific patients, scheduling implementation time, securing colleague support or adapting protocols. These actions signal genuine preparation, not just good intentions.
- Execution Quality
Execution quality signals identify what happens on a clinician's first real-world attempt and are likely the most overlooked of the predictive signals. Traditional measurement often ignores this critical moment, yet it determines whether initial action leads to sustained practice change or abandonment. Early execution quality reveals friction points that only become visible in practice. Did the clinician encounter unexpected workflow conflicts? Were patients more complex than training scenarios suggested? Did colleagues raise concerns not addressed in education? These insights are essential for refining both educational design and implementation support, yet they're rarely captured systematically in CE/CPD.
Why This Framework Matters for CEHP Designers
The implications of these critical signals are profound. Taken together, these signals reveal the human drivers of action, including confidence, intent, preparation, and early execution, that applied learning can directly influence. The ALET™ Blueprint offers a fundamental reorientation to how we can think about designing for impact and effectiveness in CPD. For example, when we measure readiness, progression and early execution within CPD, a radically clearer picture of the real-world impact of the education is seen through leading indicators that are evident long before lagging indicators, such as claims data or large-scale outcomes. These signals may offer insight into the learners’ progression toward application of learning in practice, as well as where learning may be stalling or where barriers persist.
Such signals include:
- Can the clinician actually do this in their real-world context?
- Are clinicians building momentum toward application readiness, moving from belief to preparation?
- Where are clinicians stalling when they first try to apply what they’ve learned?
- What support actually accelerates action in the clinical setting?
With careful attention to the continuum of components across the ALET™ Blueprint, there is a progression of measures that are the drivers of action.
The Path Forward: Evolving the Ways We Think About Measurement Together
Ongoing ALET™ efforts have emphasized that evolution in areas critical for CE/CPD cannot happen in isolation. This is fundamentally collective work. The solutions won't be built by any one organization, any one discipline or any one perspective.
The transition from learning-focused to enablement-designed CE/CPD represents more than methodological refinement. This is a fundamental rethinking of what we're trying to achieve and how we know when we've succeeded. Traditional metrics remain essential; they form the foundation. But if we're designing for readiness and enablement, our measurement must transform purposefully to meet this ambition.
References
- Paynter N, Pardo C, Doyle-Scharff M, et al. The Education We Deliver Isn't Built for the Change We Expect. 2025: https://aletcollaboratory.org.
- Pardo C, McGowan B, & Balmer J. Webinar recording: What Should We Measure Now? 2025. https://aletcollaboratory.org/resources
- Moore DE Jr, Green JS, & Gallis HA (2009). Achieving desired results and improved outcomes: Integrating planning and assessment throughout learning activities. J Contin Educ Health Prof., 29(1):1-15.
Interested in this article? Join the discussion on the Alliance Community.

Caroline O. Pardo, PhD, CHCP, FACEHP, is chief learning officer and co-founder of StitchedHealth and co-founder of Integrated Action Science. Dr. Pardo is a medical sociologist with 20 years of experience in education, research and implementation science.

Nancy Paynter, MBA, CHCP, is chief strategy officer and co-founder of StitchedHealth, where she leads applied learning and evidence translation strategies designed to accelerate the adoption of evidence-based care. She has more than 20 years of leadership experience across medical affairs and commercial strategy at Pfizer, Genentech and Gilead.

Jann Balmer, PhD, RN, FACEHP, FAAN, holds broad expertise and knowledge in continuing education in the health professions, nationally and internationally, including extensive work in strategic planning, capacity building and organizational change, leadership development, adult learning, educational design, institutional and organizational assessment, and innovative educational modalities that foster collaborative approaches to learning, performance and outcomes.

Brian McGowan, PhD, FACEHP, is a noted CEHP leader with combined experience as a biomedical scientist and educator leading to a career and a passion for medical education and healthcare improvement.
 Maureen Doyle-Scharff, PhD, MBA, FACEHP, is a visionary change agent who is an expert in brokering public-private partnerships that drive changes in the global healthcare ecosystem. Recently retired from Pfizer Inc, she spent nearly 25 years leading a cross-functional team focused on enabling healthcare communities to advance science and close gaps in care through independent and collaborative grants and partnerships. In addition, she spent the last few years leading Pfizer’s Institute of Translational Equitable Medicine (ITEM), focused on the science behind health disparities and translating new data and information to improve patient outcomes globally.
Maureen Doyle-Scharff, PhD, MBA, FACEHP, is a visionary change agent who is an expert in brokering public-private partnerships that drive changes in the global healthcare ecosystem. Recently retired from Pfizer Inc, she spent nearly 25 years leading a cross-functional team focused on enabling healthcare communities to advance science and close gaps in care through independent and collaborative grants and partnerships. In addition, she spent the last few years leading Pfizer’s Institute of Translational Equitable Medicine (ITEM), focused on the science behind health disparities and translating new data and information to improve patient outcomes globally.