
This is the first in a series of six articles that will describe the foundation of evidence and thinking that served as catalyst for the development and evolution of the Applied Learning and Evidence Translation (ALET™) Blueprint first described in 2025 White Paper titled “The Education We Deliver Isn't Built for the Change We Expect,”1 developed by the ALET™ Collaboratory.
Despite unprecedented investment in healthcare education and clinical decision support, the translation of evidence into practice remains critically delayed. A landmark study showed just 55% of patients receive recommended care, a number that hasn't substantially improved despite massive investment.2 This persistent gap is not best explained by a lack of information or professional intent. It reflects a missing mechanism in how we design for evidence to become action in real-world care. The Applied Learning and Evidence Translation (ALET™) Blueprint was first disseminated in 2025 as an interdisciplinary framework to address the persistent knowing-doing gap in clinical practice. By integrating behavioral, decision, network and implementation sciences, the ALET™ Blueprint challenges the traditional assumption that knowledge transfer alone drives behavior change and instead focuses on enabling confident clinical action through an eight-stage enablement architecture. In 2026, as information becomes increasingly accessible at scale, the case for ALET™ strengthens. Not because information solves translation, but because information-at-scale risks drowning clinicians in data unless we intentionally design the enablement pathway that turns knowing into action. This framework offers continuing education professionals a timely and evidence-based approach to accelerating clinical translation and improving patient outcomes.
The Translation Crisis in Healthcare Education
The healthcare industry allocates $10 to $12 billion annually to clinical education beyond graduate training3, yet this substantial investment yields a sobering return, with at least one analysis showing only a small fraction (~11%) of practicing clinicians sustained behavior change following intervention.4 This stark reality exposes a fundamental flaw in our approach to professional development and clinical education. While the field has made significant advances in content delivery methods, learning technologies and educational design, the average time from research publication to clinical implementation continues to span years, if not decades.
For continuing education professionals, this translation gap represents both a professional challenge and a call to action. Traditional approaches to clinical education have operated under the assumption that better knowledge delivery would naturally lead to improved clinical practice. However, accumulating evidence suggests that the bottleneck lies not in what clinicians know, but in their ability to confidently translate that knowledge into action within the complex, uncertain and high-stakes environment of clinical care. The Applied Learning and Evidence Translation (ALET™) Blueprint was purposefully designed as a response to this fundamental misalignment between educational intervention and clinical reality.1
In plain terms, the education community has built sophisticated ways to deliver information and even prompt action, yet the “messy middle” remains under-designed. This is the space where clinicians must integrate evidence with patient complexity, uncertainty, workflow constraints and local norms. ALET™ was formed to address where translation repeatedly stalls, regardless of modality, channel or setting, and to address the gap caused by too many approaches stopping at understanding or competence when the true goal is action in practice.
Currently, this is even more strategically important: Information-at-scale solutions can meaningfully accelerate clinician access to evidence. The risk is that we become enamored with faster knowing and mistake it for progress on adoption, when science and real-world experience show that “knowing” has never reliably produced “doing” alone. Without deliberate design for enablement, we simply reach the same stall point sooner. Our foundational purpose for developing the ALET™ Blueprint was threefold:
- To challenge the assumption that knowledge transfer equals behavior change
- To demonstrate how integrating behavioral, decision, network and/or implementation sciences multiplies clinical engagement impact
- To provide actionable pathways for accelerating clinical translation
The ALET™ Blueprint: Reframing the Problem
The ALET™ Blueprint represents a fundamental reframing of the clinical education challenge. Rather than asking how to transfer knowledge more effectively, it poses a different question: How do we enable confident clinical action? This shift acknowledges that the true barrier to practice change lies in the space between understanding and action, a space characterized by complexity, uncertainty, competing priorities, and the psychological demands of clinical decision-making.
If the goal is evidence-based decisions showing up in care, then the object of design cannot be knowledge transfer alone. The object of design must include the applied, contextual work that enables clinicians to act, especially when they face the practical question: How do I apply this evidence safely and effectively for this patient, in this setting?
The framework integrates four scientific disciplines to address this enablement gap:
- Behavioral science illuminates the psychological factors that influence clinical decision-making, including cognitive biases, decision fatigue, and the role of confidence in action.5
- Decision science provides insights into how clinicians navigate uncertainty and complexity, particularly when guidelines conflict or evidence is ambiguous.6
- Network science reveals how peer influence, professional relationships and organizational culture shape adoption patterns.7
- Implementation science offers practical frameworks for translating evidence into sustainable practice change within real-world clinical settings.8
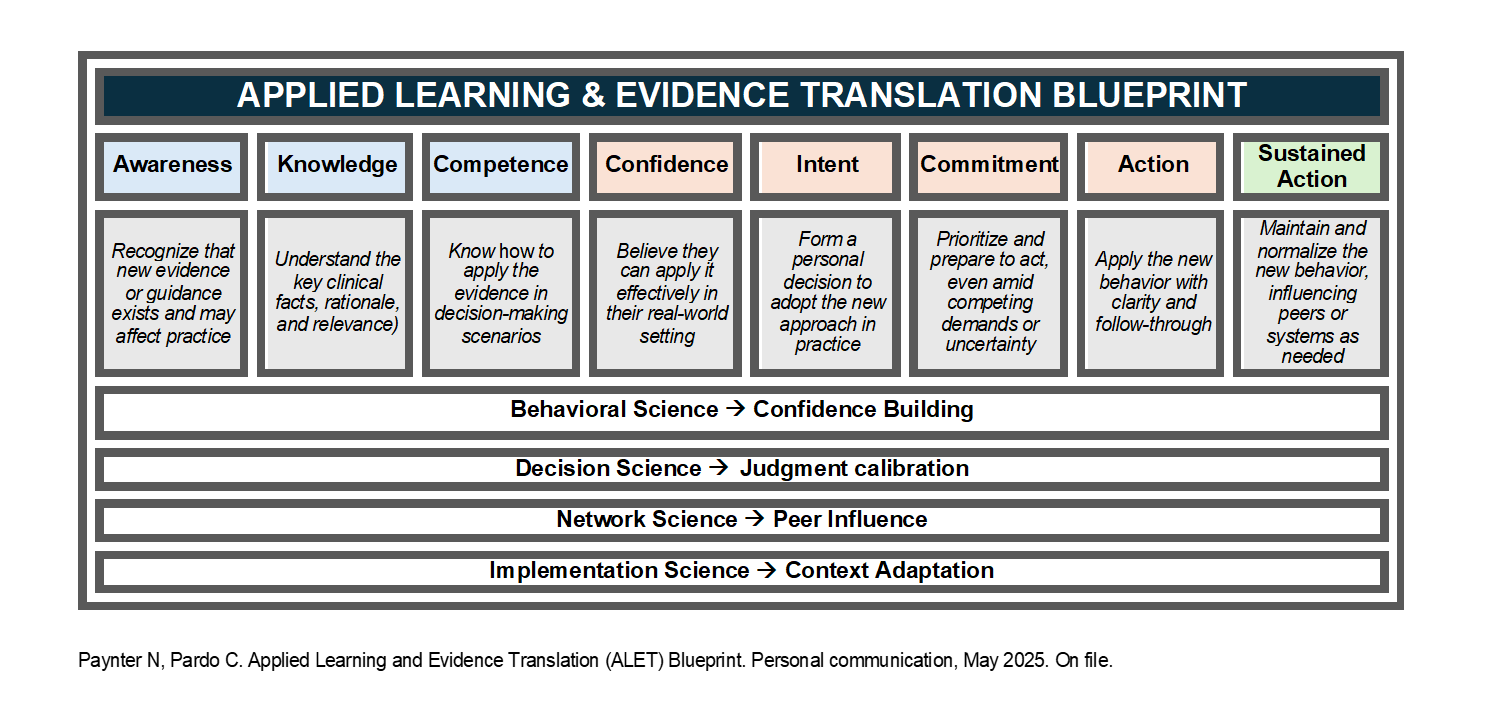
The ALET™ Blueprint integrates these sciences purposefully into a single framework focused on the enablement stages that traditional clinical education often underserves. This is what makes ALET™ a prescient innovation: ALET™ operationalizes a science-backed pathway for applied clinical translation at a time when the ecosystem is still largely optimizing information delivery. Central to the ALET™ Blueprint is its eight-stage enablement architecture, which maps the journey from awareness to integrated practice (see below). This framework recognizes that each stage presents distinct barriers and requires targeted interventions. By measuring progression through the stages, particularly confidence and commitment, and identifying specific drop-off points, continuing education professionals are better enabled to design interventions that address the actual barriers clinicians face rather than those we assume they face. Early data on the application of the ALET™ Blueprint in research is showing the model to be an effective design framework for evidence translation intervention design and evaluation.9
The Urgency of Action
Transformation windows in healthcare systems are typically narrow, as we see time frames of 18-24 months before organizations lock into new patterns of behavior and cultural integration. This temporal constraint demands that continuing education professionals act with both urgency and precision. The current moment presents a unique opportunity: Heightened awareness of healthcare quality gaps, increasing pressure for value-based care, growing recognition of implementation science, and widespread acknowledgment that traditional educational approaches require fundamental reimagining culminate in both the need and the potential for education to be designed for the change we seek to see in clinical practice.
The temptation in 2026 is to treat information-at-scale as the solution. It is a meaningful advancement, but if we allow it to reinforce the misdiagnosis that information provision is the primary constraint, we will simply reproduce the same outcomes with better tools. The opportunity now is to apply these front-end advances as leverage to invest in the enablement pathway that reduces time to evidence-based decisions by supporting clinicians through uncertainty and local constraints.
However, seizing this opportunity requires a shift in how we measure success. Rather than relying solely on traditional metrics like completion rates, satisfaction scores or knowledge assessments, we must measure confidence, self-efficacy and progression through enablement stages. These metrics have demonstrated predictive validity for behavior change and provide actionable insights for intervention refinement. Moreover, they align measurement with the actual goal of continuing education: not to inform, but to enable clinical action that improves patient care.
Conclusion: A Call to Collaborative Action
The ALET™ Blueprint offers continuing education professionals a framework grounded on established sciences for addressing healthcare's persistent knowing–doing gap. Its interdisciplinary approach acknowledges the complexity of clinical behavior change while providing practical tools for intervention design, implementation and evaluation.
The ALET™ Blueprint provides both a diagnosis of why current approaches fall short and a prescription for more effective intervention. As continuing education professionals, we have both the opportunity and the obligation to embrace frameworks that align our efforts with the goal of improving the quality of care and outcomes for patients. The moment for fundamental transformation is now.
References
- Paynter N, Pardo C, Doyle-Scharff M, et al. The Education We Deliver Isn't Built for the Change We Expect. 2025: https://aletcollaboratory.org.
- McGlynn EA, Asch SM, Adams J, et al. The Quality of Health Care Delivered to Adults in the United States. N Engl J Med. 2003;348(26):2635-2645.
- Michie S, Van Stralen MM, West R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implementation Sci. 2011;6(1):42.
Interested in this article? Join the discussion on the Alliance Community.

Caroline O. Pardo, PhD, CHCP, FACEHP, is chief learning officer and co-founder of StitchedHealth and co-founder of Integrated Action Science. Dr. Pardo is a medical sociologist with 20 years of experience in education, research and implementation science.
 Nancy Paynter, MBA, CHCP, is chief strategy officer and co-founder of StitchedHealth, where she leads applied learning and evidence translation strategies designed to accelerate the adoption of evidence-based care. She has more than 20 years of leadership experience across medical affairs and commercial strategy at Pfizer, Genentech and Gilead.
Nancy Paynter, MBA, CHCP, is chief strategy officer and co-founder of StitchedHealth, where she leads applied learning and evidence translation strategies designed to accelerate the adoption of evidence-based care. She has more than 20 years of leadership experience across medical affairs and commercial strategy at Pfizer, Genentech and Gilead.