
This is the third in a series of six articles that will describe the foundation of evidence and thinking that served as catalyst for the development and evolution of the Applied Learning and Evidence Translation (ALET™) Blueprint first described in 2025 White Paper titled “The Education We Deliver Isn't Built for the Change We Expect,”1 developed by the ALET™ Collaboratory. Please check out the first article, Bridging the Knowing-Doing Gap: The Applied Learning and Evidence Translation (ALET™) Blueprint for Clinical Behavior Change, and the second article, What Should We Measure Now? How Collaborative Community Dialogue is Evolving a Shared Framework for What Actually Drives Clinical Behavior Change.
The gap between what clinicians learn and what they actually do remains one of the most persistent challenges in continuing education in the health professions (CEHP). This gap is not new. The familiar progression from awareness through knowledge, competence, performance and ultimately to sustained action has formed the backbone of learning frameworks in CEHP. Moore et al.'s outcomes framework offered our field a practical tool for describing this journey.1 Yet too often, the stages in this framework have been treated as passive markers or “boxes to check” regarding clinicians’ exposure to education or improvement in knowledge, rather than active steps across a learning journey to applied action in practice, each of which require distinct cognitive, emotional and behavioral readiness.
What if, instead of simply measuring whether a clinician reaches a particular stage, we asked a more fundamental question: What must a clinician be able to do at each point along this learning journey to be able to apply what they learn?
This is why the ALET™ Blueprint was designed: not as another model but as a framework for CEHP professionals to design and build learning activities that are more likely to be applied accurately and sustainably applied in clinical practice.2
The Framework Versus Template Problem
When Moore and colleagues introduced the outcomes framework to the CEHP community, it was recognized widely as a valuable, structured way to think about educational design and impact across a continuum.1 It was designed as a framework, which is a flexible tool for thoughtful planning and holistic assessment. Yet in practice, the strong work by Moore et al has been reductively used as a template, or a checklist by which CME/CE developers indicate the level their program aims to achieve based on learning goals.
This distinction matters more than it might initially appear. Used as a template, the work by Moore et al. becomes a compliance exercise. Program planners identify a target level (typically knowledge or competence) and design activities to reach that endpoint. The framework gets reduced to a static measurement tool rather than a dynamic planning instrument. This approach does have benefits, such as enabling a shared language and alignment of goals across the CEHP community. But it shortchanges both the work and the full potential of what the framework offers.
The framework’s real value emerges when we use it as a planning tool: to identify gaps we aim to close, to design learning experiences that move clinicians across the continuum of stages, and to measure how effectively we've facilitated that progression toward improved, confident, sustained action. A framework requires thoughtful, purposeful effort. A template enables programming that may be neither targeted nor optimally impactful.
Reframing “Stages” as Jobs to Be Done
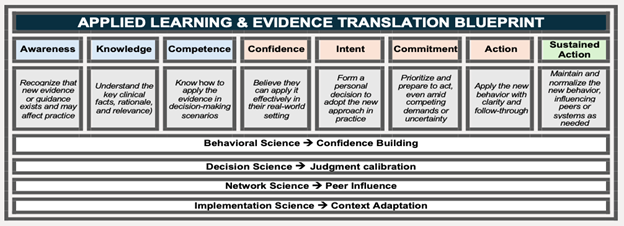
The shift is this: design CME/CE by treating each stage of learning as a distinct job to be done, something the clinician learner must achieve or experience to move forward and align measurement to each stage. The shift may seem subtle, but it is strategic. Here is how that could look across the continuum:
Awareness is only the starting point. Clinicians must recognize the relevance of the content to their own work context. The job to be done is helping them see how this applies to their patients, their practice patterns and their constraints.
Knowledge and Competence similarly require reframing. Within the knowledge stage, clinicians understand more than recall facts, as they understand what matters in their specific clinical context. And in the competence stage, they must know how to apply this information in clinical decision-making under the messy, time-pressured conditions of real practice. The job to be done is more than knowledge and skill acquisition, to include understanding and enablement for contextualized application.
Confidence is more than self-assessed comfort; confidence is better described as a clinician’s belief that they can act effectively in their own real-world context. A clinician might be competent in interpreting a diagnostic algorithm but lack confidence to use it when it contradicts their more experienced colleague's approach or when system or other constraints make the ideal pathway difficult. Designing for self-efficacy is therefore critical to the application of learning.
This reframing is not merely semantic. If we want clinicians to behave differently in practice, we need to design for their ability to recognize, interpret, decide and act. Each stage represents a capability shift that requires intentional learning design.
The Stall Beyond Competence
As prior ALET™ work has documented, activation of learning in real-world practice consistently stalls beyond competence.1 This pattern appears across specialties, practice settings and educational interventions. Clinicians gain knowledge, demonstrate competence and then the translation to sustained practice change fails to materialize. Why? Because the stages beyond competence, which include confidence, motivation, intent, commitment, and action, operate on different mechanisms than knowledge acquisition. They are not primarily cognitive challenges; they’re behavioral, social and contextual. Unfortunately, most CME/CE is not designed for these stages.
The ALET™ Blueprint offers a scaffold for education designers to work through these successive stages where implementation typically stalls. It provides a planning framework for identifying what the next steps would be to move learners through confidence (Can I do this in my setting?), motivation (Do I want to? Do my attitudes and beliefs align and support this step?), intent (Will I plan to?), commitment (Am I ready to overcome barriers?) and action (Am I actually doing it?).
This scaffold aligns with how clinicians learn when the aim is to change practice. They need to take evidence, test it, refine their application, gain confidence through experience and practice over time. CPD should offer safe spaces for this progression or opportunities to rehearse, receive feedback, troubleshoot barriers and build the behavioral momentum needed for sustained change. The ALET™ Blueprint is purposefully aimed at designing education to facilitate movement across this continuum and to guide measurement along the continuum.
Engineering the Bridge, Not Just Measuring the Gap
The strategic value of the ALET™ Blueprint is that it offers a framework for intentionally designing education around these capability shifts to build CEHP for reliable translation of learning into practice. By integrating the sciences of behavior change, implementation, and learning, ALET™ enables CEHP professionals with an engineering framework to bridge learning to sustained clinical action.
If we want to make credible claims that our educational intervention led to practice change, we need learning that is purposefully designed to address these relevant stages. If CEHP is not designed to move clinicians through the stages following competence and measuring the discrete steps along the path, how can we credibly claim causation for moving them to action? The more rigorous approach to measure across these stages is to ensure the learning design was built to address each transition point. A latent benefit of such designs is that they will yield data showing not just whether change occurred, but where programs were effective and where effectiveness stalled. This gives us actionable insights for future CEHP interventions to close remaining or persistent gaps.
The Work of Thoughtful Implementation
None of this happens automatically. The ALET™ Blueprint is not a plug-and-play solution. Like all true frameworks, it requires genuine work to be implemented effectively.
This work involves:
- Understanding not just what clinicians need to know, but what capabilities they need at each stage to progress
- Selecting educational approaches specifically matched to the stage transitions we are trying to facilitate
- Assessing not just outcomes at a single endpoint, but progression across the continuum
- Using data about where learners stall to improve future programming
Working through each stage may sound daunting. But consider the alternative: Continuing to build education that reliably produces knowledge and competence but inconsistently generates practice change should no longer be acceptable as an end goal.
The Next Evolution of the Learning Continuum
The stages of the learning continuum have been described by learning science experts and others through an evolving body of literature.1 We know that clinicians progress from awareness through action, and models have been built to describe this journey. What the ALET™ Blueprint adds is a scaffolding for addressing the behavioral and contextual challenges where activation stalls offer a methodological plan for designing for practice change. This is framework work, not template work. For our field, which is committed to educational impact, this work is aligned to our core mission.
References
- Moore DE Jr, Green JS, & Gallis HA (2009). Achieving desired results and improved outcomes: Integrating planning and assessment throughout learning activities. J Contin Educ Health Prof., 29(1):1-15.
- Paynter N, Pardo C, Doyle-Scharff M, et al. The Education We Deliver Isn't Built for the Change We Expect. 2025: https://aletcollaboratory.org.
- Pardo C, McGowan B, & Balmer J. Webinar recording: What Should We Measure Now? 2025. https://aletcollaboratory.org/resources
Interested in this article? Join the conversation in the Alliance Community.
.png?ver=BAfj-MQcR8Q556cB5EDmKA%3d%3d) Caroline O. Pardo, PhD, CHCP, FACEHP, is chief learning officer and co-founder of StitchedHealth and co-founder of Integrated Action Science. Dr. Pardo is a medical sociologist with 20 years of experience in education, research and implementation science.
Caroline O. Pardo, PhD, CHCP, FACEHP, is chief learning officer and co-founder of StitchedHealth and co-founder of Integrated Action Science. Dr. Pardo is a medical sociologist with 20 years of experience in education, research and implementation science.
.png?ver=LTKUIW9fm-l2row3AWvjWw%3d%3d) Nancy Paynter, MBA, CHCP, is chief strategy officer and co-founder of StitchedHealth, where she leads applied learning and evidence translation strategies designed to accelerate the adoption of evidence-based care. She has more than 20 years of leadership experience across medical affairs and commercial strategy at Pfizer, Genentech and Gilead.
Nancy Paynter, MBA, CHCP, is chief strategy officer and co-founder of StitchedHealth, where she leads applied learning and evidence translation strategies designed to accelerate the adoption of evidence-based care. She has more than 20 years of leadership experience across medical affairs and commercial strategy at Pfizer, Genentech and Gilead.
 Maureen Doyle-Scharff, PhD, MBA, FACEHP, is a visionary change agent who is an expert in brokering public-private partnerships that drive changes in the global healthcare ecosystem. Recently retired from Pfizer Inc, she spent nearly 25 years leading a cross-functional team focused on enabling healthcare communities to advance science and close gaps in care through independent and collaborative grants and partnerships. In addition, she spent the last few years leading Pfizer’s Institute of Translational Equitable Medicine (ITEM), focused on the science behind health disparities and translating new data and information to improve patient outcomes globally.
Maureen Doyle-Scharff, PhD, MBA, FACEHP, is a visionary change agent who is an expert in brokering public-private partnerships that drive changes in the global healthcare ecosystem. Recently retired from Pfizer Inc, she spent nearly 25 years leading a cross-functional team focused on enabling healthcare communities to advance science and close gaps in care through independent and collaborative grants and partnerships. In addition, she spent the last few years leading Pfizer’s Institute of Translational Equitable Medicine (ITEM), focused on the science behind health disparities and translating new data and information to improve patient outcomes globally.