Introduction
The Patient Centered Medical Home (PCMH) represents a model that serves to improve healthcare by transforming how primary care is organized and delivered.1 The Agency for Healthcare Research and Quality (AHRQ) ascribes five functions and attributes to what constitutes a PCMH:1
- Patient-centered – provision of care that is a relationship-based partnership with the patient requiring understanding and respecting each patient’s unique needs, culture, values, and preferences while ensuring an orientation toward the whole person.
- Comprehensive care – a practice comprised of a team of care providers that meet the large majority of each patient’s physical and mental healthcare needs, including prevention and wellness, acute care, and chronic care.
- Coordinated care – coordinates care across all elements of the broader healthcare system, including specialty care, hospitals, home healthcare, and community services.
- Accessible services – provides more access to services including shorter wait times for urgent needs, enhanced in-person hours, 24/7 telephone or computer access to a member of the care team, and alternative methods of communication (eg, email, text).
- Quality and safety – commitment to quality improvement by ongoing engagement in activities such as using evidence-based medicine and clinical decision-support tools to guide shared decision making with patients and families, engaging in performance measurement and improvement, measuring and responding to patient experiences and patient satisfaction, and practicing population health management.
In many respects, these attributes are not the norms of modern primary care and primary care practices undergoing transformation toward a PCMH require a supporting infrastructure of education and resources that has not previously existed. To enable this transformation, there has been a great need for the creation of standardized processes that allow these practices to assess all facets of the patient experience and the approach to care.
The National Committee for Quality Assurance (NCQA) has developed that standardized approach, and together with Med-IQ and ArcheMedX have created a new educational model that focuses on linking medical knowledge to enhancements to the practice processes involved in quality care.
NCQA
NCQA is a private, 501(c)(3) not-for-profit organization dedicated to improving health care quality. Since its founding in 1990, NCQA has been a central figure in driving improvement throughout the health care system, helping to elevate the issue of health care quality to the top of the national agenda.
NCQA’s Patient-Centered Medical Home Recognition Program is the most widely adopted Patient-Centered Medical Home evaluation program in the country. As of August of 2017, the program has recognized over 12,800 practices as PCMHs representing over 61,000 clinicians.
NCQA’s PCMH Recognition Program aligns with the ARHQ definition of a PCMH, specifically organized around the following standards:
- Patient-Centered Access and Continuity – Guides practices to provide patients with convenient access to clinical advice and helps ensure continuity of care.
- Team-Based Care and Practice Organization – Helps structure a practice’s leadership, care team responsibilities, and how the practice partners with patients, families and caregivers.
- Knowing and Managing Your Patients – Sets standards for data collection, medication reconciliation, evidence-based clinical decision support and other activities.
- Care Management and Support – Helps clinicians set up care management protocols to identify patients who need more closely managed care.
- Care Coordination and Care Transitions – Ensures that primary and specialty care clinicians are effectively sharing information and managing patient referrals to minimize cost, confusion and inappropriate care.
- Performance Measurement and Quality Improvement – Helps practices develop ways to measure performance, set goals and develop activities that will improve performance.
Strategies for Success as a PCMH – An Overview
NCQA has identified attributes that contribute to PCMH success:
- Technical assistance to help create and sustain the transformation. Practices value practical examples and support for pursuing the medical home model of care.
- A systems approach to QI that results in data, standard measurements and technical assistance.
In 2015, NCQA partnered with Med-IQ and ArcheMedX to develop the Strategies for Success as a Patient-Centered Medical Home pilot initiative. This program offered support in the NCQA-identified areas in order to help practices maintain and improve their quality of care. A mix of live and learner accessible activities for the health care team was designed so care teams could select topics that related directly to their patient population and target areas for quality improvement. The disease specific quality improvement activities were linked to the PCMH model, with feedback provided specifically for PCMH requirements. This “ladders up” to the triple aim of better quality, cost and patient experience.
Strategies for Success became the first initiative of its kind to focus the education on the entire patient care team, including both clinical and non-clinical members of the practice satisfying the need for certified education and unique practice support interventions.
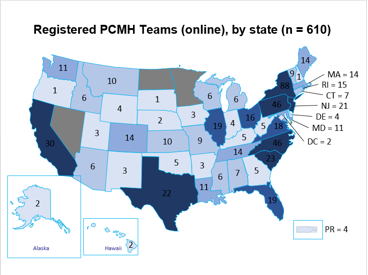
Phase one of the Strategies for Success initiative was comprised of 10 full-day, certified workshops, 12 online certified interactive activities employing the ArcheMedX ArcheTeam platform, four NCQA PCMH Best Practices publications, and the provision of multiple patient engagement tools. Combining clinical education on topics such as comprehensive diabetes management, reducing cardiovascular risk factors, managing lower urinary tract symptoms, obesity, and symptoms of depression, and improving age cohort-based hepatitis C testing and HIV screening in at-risk populations, with practice-based process improvement to date, Strategies for Success has enrolled over 600 practices and 2,000 individuals (both clinical and non-clinical staff) into the program.
The Strategies for Success series is unique in that it combines traditional clinical learning objectives with larger practice-based objectives and objectives specific to PCMH recognition. Clinical objectives are similar to those seen in traditional CE activities geared toward improving knowledge and competencies related to clinical topics. Measurable, practice-based objectives focus on engaging patients in shared decision-making, discussions on lifestyle modifications to improve overall health, implementation of processes to involve multiple members of the care team in patient assessment and monitoring, and development of quality improvement goals for the practice.
The value of the Strategies for Success model lies in the ability for activities to be taken individually or together as a team. The shared learning experience enables users to view, download, and recommend practice-based tools and to engage in team discussions about how to best apply evidence-based approaches to their practice. Additionally the series offers practice management tips and suggestions for optimizing care helping the team communicate more effectively and enhance patient outcomes.
What We’ve Learned
The transformation to a PCMH model requires ongoing team-based engagement and blended clinical- and process-oriented focused education as well as strategies that enhance communication and care coordination. It also requires a transformation toward and a commitment to continuous quality improvement.
The Strategies for Success Phase 1 Experience:
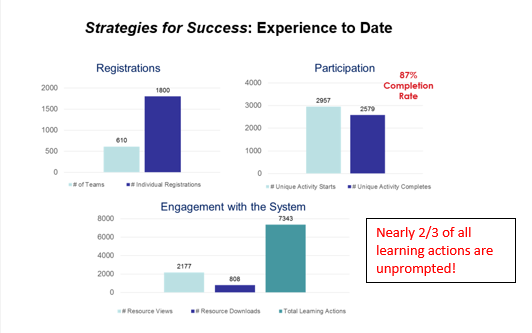
This pilot experience educating and communicating with the PCMH community suggest that this model unique supports learner and team engagement and prior evidence suggests that the level of engagement within the ArcheMedX Learning Actions Model is directly related to the effectiveness of the educational interventions. And, in fact, Strategies for Success has led to significantly positive changes in knowledge, attitudes, and competence.
Observed Improvements
|
Disease State
|
Practice change commitments
|
|
Diabetes
|
Broader assessment of patients not at A1C goal
|
|
HCV screening
|
Improvements in age cohort-based testing
|
|
Obesity management
|
Developing personalized management plans
|
|
Reduction of CV risk factors
|
Increases in assessment of 10-year cardiovascular disease (CVD) risk
|
|
Management of LUTS
|
Enhancement of dialogue between provider and patient on identification of symptoms
|
|
Management of depression
|
Increases in utilization of depression screening tools
|
Patient Impact
On average, post-activity learning gains were measured for 46% of clinicians (MD, DO, PA, NP, RN and LPN). Looking only at these clinicians, estimated patient impact per clinical focus is detail in the table below.
|
Clinical focus
|
% of participating clinicians with post-activity learning gains (total number of clinician participants)
|
Estimated patient impact
|
|
OAB
|
43% (120)
|
2550 patients with lower urinary tract symptoms and/or OAB
|
|
Diabetes
|
47% (251)
|
33,040 patients with diabetes
|
|
Obesity
|
48% (217)
|
63,000 patients either obese or at an unhealthy weight that requires intervention
|
|
HCV
|
42% (218)
|
23,000 patients that should be screened for HCV
|
|
Depression
|
56% (199)
|
11,200 patients with depression
|
|
CVD
|
41% (204)
|
29,050 patients with dyslipidemia
|
Educational Effect:
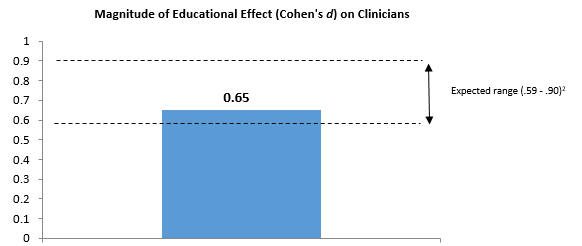
Learning gains were assessed via single correct answer multiple choice questions administered to matched clinicians (MD, DO, PA, NP, RN and LPN) pre- and post-activity.
The aggregate magnitude of educational effect (Cohen’s d) across all twelve activities was .65 (see Figure). This medium-sized effect2 approximates what has been reported in recent meta-analyses for knowledge gains associated with participation in Internet-based learning activities assessed by similar non-randomized methods.3 The largest learning gains were measured for the depression (d = .82) and obesity (d = .80) activities.
Moving Forward: Strategies for Success Phase 2
Along with the on-going outcomes analysis and research into the impact of the pilot Strategies for Success program, the collaborators have continually assessed how the interventions and practice support could be further enhanced. These insights have fueled plans for phase two of the program, or Strategies for Success 2.0.
This next phase in the initiative’s evolution will be guided by a steering committee that includes nationally recognized clinical faculty as well as NCQA’s PCMH Certified Content Experts (CCEs), who are well versed in the application of PCMH standards in a primary care setting along with specific feedback from high-participation learners and practices. In brief, Strategies for Success 2.0 will provide practices with continuous engagement over time, reinforcement of the learning, focusing on more rapid dissemination of best practices, and opportunities for live interaction with the experts. This will provide patient-centered practices with a foundation that supports achievement of identified standards and provides a bridge to the development of future quality improvement initiatives.
The components of this proposed series include:
- More accessible live webinars – focusing on reviews of clinical topics ranging from diagnosis to treatment, and how to engage in clinical care in the context of existing quality measures. These webinars will also provide best practices discussions on overcoming common barriers and creating team-focused discussions on the roles of each in various problem-solving scenarios.
- Extension of ArcheViewer-powered curriculum – addressing new topics and diving more deeply into previously covered topics
- ArcheTeam-enabled continuous engagement via Rich Content Posts (RCPs) – RCPs will be used to provide on-going and consistent reinforcement of the learning in the live/enduring webinars by constructing various learning experiences in a manner that allows for a more personalized experience and affords the collaboration the opportunity to post content in a more responsive fashion. RCPs will include interviews with clinical faculty, process experts, PCMHs who have developed best practices, and team-based exercises and case challenges across a variety of clinical topics.
The proposed Strategies for Success expansion is estimated to launch in the Spring of 2018 and endure for 24 months.
Conclusion:
Taken as a whole, the Strategies for Success initiative allows for cross-pollination and deeper, more engaged learning, enhancing the Collaboration’s ability to serve primary care clinicians and their care teams working within or striving toward a patient-centered practice model. The proven success of the model to date demonstrates that for the PCMH model to be successful, dedicated and continuous education and engagement is needed to sustain practices transformation toward quality. Most importantly, these lessons highlight new ways of envisioning the interventions we, as a community of educators, must provide. We must see beyond an individual learner and understand how our interventions may be designed to support each learner AND the teams and systems in which they practice.
*Note: The project discussed in this article received educational grants from AbbVie Inc., Allergan, Inc., Amgen, Astellas Pharma US, Inc., AstraZeneca, Gilead Sciences, Inc., Lilly USA, LLC, Sanofi-aventis U.S. Inc. and Regeneron Pharmaceuticals, Inc., and Takeda Pharmaceuticals International, Inc., U.S. Region.
References:
- Defining the PCMH. AHRQ Patient Centered Medical Home Resource Center. Available at: https://www.pcmh.ahrq.gov/page/defining-pcmh. Accessed on September 8, 2017.
- Cohen J. (1988) Statistical power analysis for behavioral sciences (2nd ed). Hillsdale, NJ: Lawrence Earbaum Associates.
- Cook DA, Levinson AJ, Garside S, Dupras DM, Erwin PJ, Montori VM. Internet-based learning in the health professions: a meta-analysis. JAMA 2008;399:1181-1196.